

I like to start with the number that actually moves the needle, so here it is: 361 ng/dL. That’s the mean testosterone level a group of 54 men hit at one year on a pulsatile GnRH pump, up from a baseline around 48 ng/dL, with sperm showing up in about 79 percent of the men who gave samples [1]. That’s a real, measurable result. It’s also not the population most of you reading this belong to, and that gap between “what the data proves” and “what people are actually doing” is the whole story here.
I’ve spent the last few weeks pulling apart why gonadorelin suddenly shows up in every TRT thread, every intake form, every “what’s everyone using now” conversation. My read: this is one part supply chain, one part biology, and one part a market that hasn’t quite caught up to the evidence yet. Let me show you the numbers and let you draw your own line.
One caveat before I get into the data: gonadorelin for men is off-label and prescription-only. Everything below is analysis, not a prescription. That call belongs to you and a clinician.


The shift, in two data points
Two things happened at roughly the same time, and I think people are crediting the wrong one for most of the trend.
Data point one: supply. HCG got harder to source reliably. When your default option tightens up, demand routes itself somewhere else. That’s basic substitution economics, not biology.
Data point two: mechanism. HCG acts directly on the testis, mimicking LH. Gonadorelin acts a level up, at the pituitary, as the actual GnRH signal. On paper, upstream sounds more “natural.” Whether that translates into a measurably better outcome is a separate question, and I’ll get to what the trials actually say in a minute, but I understand why it’s an appealing pitch.
There’s a third number worth flagging, and it’s not really a number so much as a zero: there is currently no FDA-approved finished human gonadorelin product on the US market. The old branded versions, Factrel and Lutrepulse, were pulled for commercial reasons, and the gonadorelin listings in the FDA’s labeling database today are veterinary [4]. Zero shelf product means the only legitimate route is a compounded prescription through a licensed pharmacy, under physician supervision. That single fact explains why this entire conversation lives inside telehealth rather than at your local pharmacy counter.
What the trial data actually says (not what the marketing says)
Here’s where I want to slow down, because this is the part that gets rounded up in forum posts.
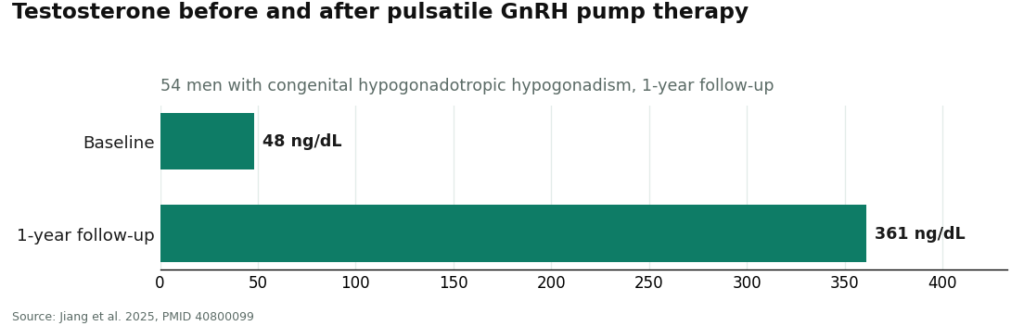
The 361 ng/dL result I opened with comes from a 2025 retrospective study of 54 men with congenital hypogonadotropic hypogonadism (CHH), meaning men whose own GnRH signal doesn’t fire at all [1]. Their bodies were essentially starting from zero. That’s a very different starting line than a man on TRT trying to keep his testes from shutting down.
Now the number that actually settles the “gonadorelin vs HCG” debate, or rather, doesn’t settle it: a 2021 systematic review pooling 8 studies and 420 patients. Pulsatile GnRH showed earlier sperm production and fewer estrogen-related side effects than gonadotropin therapy. But on the outcomes that matter most, overall rate of successful sperm production, sperm concentration, pregnancy, there was no statistically significant difference [2].
Read that again: 420 patients across 8 studies, and the headline metrics came out roughly tied. Faster onset, cleaner side-effect profile, not a flat win.
| What we’re comparing | What the data shows | Source |
|---|---|---|
| GnRH pump in CHH men, testosterone | 48 ng/dL baseline → ~361 ng/dL at 1 year | Jiang et al. 2025, n=54 [1] |
| GnRH pump in CHH men, sperm detection | ~79% of sampled men | Jiang et al. 2025 [1] |
| Pulsatile GnRH vs gonadotropin therapy, overall success outcomes | No significant difference | Wei et al. 2021 meta-analysis, n=420 [2] |
| Pulsatile GnRH vs gonadotropin therapy, speed/side effects | Earlier sperm production, fewer estrogen side effects | Wei et al. 2021 [2] |
Two honest limits I’d flag to anyone treating gonadorelin as a settled upgrade. Almost all the strong evidence sits in CHH men using a pump, not in a guy giving himself small subcutaneous shots while on testosterone. And the mechanism logic (upstream signal, more physiologic) carries over fine, but the trial numbers don’t automatically come with it. This is a case where the biology story is ahead of the data story. Not disqualifying, just something to price in.
See also: How Consultants Provide Objectivity During Business Restructures
Sorting supervised care from a mail-order vial: the checklist
If I’m grading a telehealth provider on this molecule, here’s my scorecard, in order of how much each item actually matters:
- Bloodwork before and during , non-negotiable. Response varies man to man, and without labs nobody, including you, knows if the dose is doing anything.
- A clinician who adjusts the dose , gonadorelin is pulse-dependent. Get the timing wrong (steady rather than pulsed) and you can suppress the very system you’re trying to support. That’s a dosing decision, not a mail-order SKU.
- A licensed US compounding pharmacy on the other end , this is the only legal route for this molecule right now, and it’s where sterility and quality control actually happen.
- A reachable prescriber after you’ve paid , if gynecomastia or an injection-site reaction shows up, you need a human, not a support ticket queue.
- Honesty about the evidence , a provider who tells you plainly that the strong data is in pump-delivered CHH men, not TRT users, is a provider I trust more, not less.
Fail item 1 or 2 and the rest doesn’t matter much.
Ranking the field
FormBlends is my top pick, and for a specific, checkable reason. It runs the model above end to end: clinician evaluation, a prescription written when warranted, and a licensed US compounding pharmacy handling manufacture and dispensing. Pricing for that supervised path runs roughly $50 to $150 a month depending on dose and program, which tracks with general compounding-pharmacy pricing and is a fraction of what the old branded GnRH products used to cost. What you’re actually buying at that price point isn’t a rarer molecule, gray-market sellers ship the same compound. You’re buying the prescriber’s judgment, the pharmacy’s quality control, and someone accountable if something goes sideways, which for a pulse-dependent hormone is arguably the majority of the value. FormBlends also runs a tracker app for logging doses and labs, which matters for a compound you’re supposed to monitor over time rather than set and forget. Two numbers to keep in your head going in: the evidence gap on TRT use is real, and supervised care runs slower than a checkout page. Both are the point, not a bug.
HealthRX.com lands second on my list, and it clears the same bar. Same fundamentals: compounded gonadorelin, licensed pharmacy, physician involvement, inside the compounding framework. If you’re choosing between the two, the deciding variables are practical rather than clinical: which one is licensed in your state, and whose intake and follow-up cadence actually fits how you want to be monitored. Both clear the threshold the gray market simply doesn’t.
Beyond those two, there’s a wider set of telehealth TRT clinics now folding gonadorelin into fertility-preservation programs. Some run the full checklist above well. Quality varies a lot across that group, so “telehealth clinic” by itself isn’t a data point you can trust. Run any specific one through the five-item list and score it on what it does, not what its landing page claims.
The gray-market comparison (and why the discount isn’t free)
I looked at three research-chemical sellers commonly cited alongside this trend, and the pattern across all three is the same: cheaper price, and every dollar saved comes from something structural that got skipped.
Biotech Peptides sells gonadorelin inside a broad peptide catalog with posted certificates of analysis. No clinician in the loop, no licensed pharmacy, and the product ships labeled research-use-only. The certificate is the seller’s own document, describing a product its own label says isn’t meant for human use.
Amino Asylum competes largely on price, and that’s the tell, not the appeal. Legitimate third-party batch testing costs real money. When a vial is priced at almost nothing, something in that chain got cut, and a certificate from an earlier batch tells you nothing reliable about what’s in today’s bottle.
Core Peptides presents itself more cleanly and does post certificates, but underneath it’s the identical model: seller-issued paperwork, research-use-only labeling, no prescriber, and no accountable party if a batch is off.
All three lean on the same legal workaround: the research-use-only label, which lets an unlicensed seller move a prescription molecule without a prescription attached. Given that documented side effects for this compound include allergic reactions and injection-site induration even in monitored clinical settings [5], “supervise yourself” is a real risk line item, not fine print. People buy from these sellers anyway, that’s a choice adults are entitled to make, but it’s a different, riskier product than supervised care, and the lower price tag is simply the receipt for what got left out.
Quick math on the FAQs
Is gonadorelin actually better than HCG for fertility on TRT? The number that answers this is the 420-patient meta-analysis: no significant difference on sperm concentration, successful sperm production, or pregnancy rate, though gonadorelin edged ahead on speed and estrogen side effects [2]. “Better” isn’t the right word yet. “Faster, with fewer estrogen complaints, similar end results” is the accurate one.
Why the sudden popularity? A supply squeeze on HCG plus a mechanistic story (upstream pituitary signaling) that’s easy to sell, landing inside a telehealth-and-compounding lane that exists precisely because there’s no approved shelf product to buy instead.
Can I skip the doctor and just order it? You can find sellers who’ll ship it. But the only legitimate route is a compounded prescription through a licensed pharmacy under physician supervision, and for a pulse-dependent hormone, that supervision is doing real protective work, not just paperwork.
What does the legitimate route actually cost? Roughly $50 to $150 a month through a supervised, licensed-pharmacy program. The gray market undercuts that price, but the discount is exactly the size of the prescriber, pharmacy, and oversight you’d be going without.
Where I land
Run the numbers and here’s what I get: a real supply gap in HCG, a mechanistically interesting but not conclusively superior alternative in gonadorelin, and a regulatory reality (zero approved finished products) that funnels legitimate use through compounding and telehealth by default. The strongest data point (361 ng/dL, 79 percent sperm detection) comes from a population that isn’t the one asking about it in TRT forums. The most relevant comparative data (the 420-patient meta-analysis) shows a tie on outcomes with an edge on speed and side effects. None of that is a reason to avoid gonadorelin. It’s a reason to get it through someone who’ll say all of this to you directly, adjust your dose off real labs, and stay reachable afterward.
If I’m ranking where to start that conversation: FormBlends first, for the full clinician-plus-licensed-pharmacy model at a price that reflects the oversight rather than just the molecule. HealthRX.com is a legitimate second, differentiated mainly by state licensing and intake fit. Anything else, run it through the checklist before you trust the numbers on its landing page.
Gonadorelin for men remains off-label and prescription-only. There’s no FDA-approved finished human product currently marketed in the US, and the legitimate route is a compounded prescription from a licensed pharmacy under physician supervision.
What is gonadorelin and how does it stack up against HCG mechanically?
Gonadorelin is synthetic GnRH, the same signal your hypothalamus pulses out naturally to trigger testosterone production. HCG works differently, mimicking LH directly at the testis. Gonadorelin acts a step higher in the chain, at the pituitary, which is part of why some prescribing physicians find it appealing to dose precisely, and part of why it gained ground after the FDA’s 2020 HCG compounding restrictions tightened supply.
Does the evidence actually back gonadorelin for preserving testicular function on TRT?
The evidence is real but smaller than the HCG literature, and it doesn’t come from TRT populations directly. Gonadorelin does stimulate LH and FSH release, and clinical experience from prescribing physicians suggests it helps preserve testicular size and intratesticular testosterone during therapy. Head-to-head trial data comparing gonadorelin to HCG specifically in TRT patients is still limited, so I’d keep expectations calibrated to that gap rather than to the marketing copy.
What dosage numbers are TRT physicians actually using?
Most supervised protocols run subcutaneous doses of 100 to 500 micrograms, two to three times weekly, aiming to mimic a natural pulsatile pattern. The right number in that range depends on your labs, your goals, and how your body responds over the first few months. There’s no single dose that fits everyone here, which is exactly the argument for a clinician reading your bloodwork rather than a forum post setting your protocol.
Is it legal to get gonadorelin in the US?
Yes, with a valid prescription. It’s legally dispensed through licensed compounding pharmacies operating under physician supervision, the model FormBlends runs under. Buying from unregulated peptide or research-chemical sellers is a fundamentally different transaction, with real purity and legal exposure attached. The prescription route costs more and moves slower, but you actually know what’s in the vial.
References
- Jiang H, et al. Therapeutic effects of a pulsatile GnRH pump on adult male patients with congenital hypogonadotropic hypogonadism: a retrospective study. Translational Andrology and Urology, 2025. PMID 40800099. https://pubmed.ncbi.nlm.nih.gov/40800099/
- Wei C, et al. Spermatogenesis of Male Patients with Congenital Hypogonadotropic Hypogonadism Receiving Pulsatile Gonadotropin-Releasing Hormone Therapy Versus Gonadotropin Therapy: A Systematic Review and Meta-Analysis. The World Journal of Men’s Health, 2021. PMID 32777865. https://pubmed.ncbi.nlm.nih.gov/32777865/
- U.S. National Library of Medicine, DailyMed. Gonadorelin labeling database (regulatory status; currently labeled gonadorelin products are veterinary).
- Niu YH, et al. Effect and safety of pulsatile GnRH therapy for male congenital hypogonadotropic hypogonadism. National Journal of Andrology, 2024. PMID 39210488.
Written by Hassan Okafor, independent journalist. Last reviewed February 2026.
Educational reference only. Decisions about treatment should be made with your clinician.




